Reuben Notes
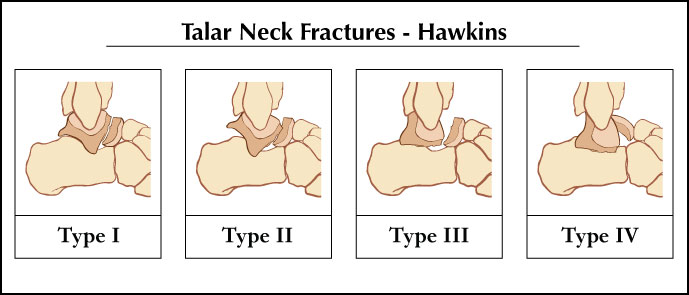
Type I: Vertical fracture of the talar neck without displacement
- disruption of 1 blood vessel
- AVN risk 12%
- Treatment: NWB short leg cast 6-8 wks. Take serial radiographs as it is important to see trabeculation across the fracture before starting weight bearing.
Type II: Vertical fracture of talar neck with dislocation of the talar body from the STJ
- disruption of 2 blood vessels
- AVN risk 42%
- Treatment: Attempt closed reduction - push backwards on plantarflexed foot while pulling forward on the distal tibia. If successful percutaneous pin. If unsuccessful even after 1 attempt - ORIF
Type III: Vertical fracture of the neck of the talus, dislocation of the STJ and ankle
- disruption of 2 blood vessels
- AVN risk 91%
- Treatment: ORIF
Type IV: Type III with addition displacement of the Talonavicular joint
- disruption of 3 blood vessels
- AVN risk 95%
- Treatment: ORIF